10/10/14 Updates.....tweets and links
Links....
Tweets.....




Zero Hedge....
 Submitted by Tyler Durden on 10/09/2014 09:12 -0400
Submitted by Tyler Durden on 10/09/2014 09:12 -0400

Links from Naked Capital.....
Brandon Smith ....
http://www.alt-market.com/articles/2354-an-ebola-outbreak-would-be-advantageous-for-globalists

Zero Hedge.....
Submitted by Tyler Durden on 10/08/2014 17:46 -0400






Submitted by Tyler Durden on 10/08/2014 08:48 -0400

Evening tweets.... 2nd case in Texas ?

Links....
Tweets.....
 Telegraph News
Telegraph News
Ebola toll passes 4,000 as fears grow worldwide http://tgr.ph/1qzNReX
 LeftfootLeeds
LeftfootLeeds
Former Border Patrol Agent: CDC "Disappearing" Potential Ebola Victims - http://fb.me/1loRvcYvs

Public Health Emergency Declared In Connecticut Over Ebola: Civil Rights Suspended Indefinitely http://www.zerohedge.com/news/2014-10-10/public-health-emergency-declared-connecticut-over-ebola-civil-rights-suspended-indef …

Passenger With Ebola Symptoms Quarantined At Las Vegas Airport http://www.zerohedge.com/news/2014-10-10/passenger-ebola-symptoms-quarantined-las-vegas-airport …

MORE THAN 200 HEALTH WORKERS HAVE DIED OF EBOLA: WHO
Suspected Ebola Patient From Guinea Admitted in Rio Hospital
Worried About "Ebolas On A Plane"? Five Things To Know http://www.zerohedge.com/news/2014-10-09/worried-about-ebolas-plane-five-things-know …
 RIA Novosti
RIA Novosti
MORE: #Russia forwards to #UN proposals on helping West African states hit by #Ebola http://bit.ly/1tJwkTC
 Progressive Warrior
Progressive Warrior
Ebola outbreak reveals massive disparities in U.S. hospital preparedness - Yahoo News http://yhoo.it/1wa6tqg

 José Pertierra
José Pertierra
Believe It Or Not, Cuba Is Providing The Most Aid For Ebola Of Any Country http://elitedaily.com/news/world/cuba-provides-ebola-aid-video/792353/ … vía @elitedaily
 Dave
Dave
"The Nightmare Scenario Is Around The Corner... Ebola Is The World's Next AIDS" http://www.zerohedge.com/news/2014-10-09/nightmare-scenario-around-corner-ebola-worlds-next-aids …
 Global Travel News
Global Travel News
#swineflu #travel Ebola UK: why screening travellers is pointless - http://Telegraph.co.uk http://bit.ly/1C0EnQ9
CDC could quarantine U.S. citizens for weeks if they refuse Ebola screenings http://news.yahoo.com/cdc-could-quarantine-u-s--citizens-for-weeks-if-they-refuse-ebola-screenings-230534518.html?soc_src=mediacontentstory … via @oknox

 Akin Unver
Akin Unver
Experts: ISIS Could Use Ebola In Bio-Terror Attack Against US -- http://washington.cbslocal.com/2014/10/09/experts-isis-could-use-ebola-in-bio-terror-attack-against-us/ …
Into the eye of the storm: US Marines arrive in Ebola hotbed of Liberia to help stop the spread of the deadly virus http://dlvr.it/792Zv2

 mike falkenstein
mike falkenstein
The CDC Is Relying on People To Tell the Truth About Contact with Ebola | @DefenseOne http://www.defenseone.com/threats/2014/10/cdc-relying-people-tell-truth-about-contact-ebola/96140/#.VDfDBXvBqZQ.twitter …

 The Guardian
The Guardian
Ebola isn’t just a health crisis – it’s a social and economic one too | Amara Konneh http://gu.com/p/42b2q/tw @commentisfree

 CERTIFIED VIRGIN
CERTIFIED VIRGIN
[The Trent Online] Ebola: Liberia Cancels Parliamentary Elections: AFP – Ebola-hit Liberia has suspended natio... http://tinyurl.com/lrkdqzt
- Photos · View all




Zero Hedge....
Ebola Pandemic Hits Germany, Turkey, And Australia As Infected Spanish Nurse Went Un-Quarantined For A Week
Despite the still confident exclamations from officials that the Ebola pandemic is 'contained', more and more nations are admitting to Ebola-symptomatic cases or bringing infected patients back from Africa for treatment. Australia has its first potential case of the deadly disease, as Bloomberg reports a nurse who returned from volunteering in Africa has developed Ebola-like symptoms. Despite claims that Nigeria's outbreak is over, a Turkish worker there has been hospitalized in Istanbul after signs of high fever and diarrhea. Health officials from Germany confirm a 3rd Ebola patient has arrived in the country - having contracted the disease in Liberia. And finally, just as in the sad case of Thomas Duncan in Dallas, The Guardian reports the infected Spanish nurse went untreated and unquarantined for a week despite reporting symptoms at least three times to hospital officials. It seems the world is ill-prepared for this...
Bloomberg reports, a nurse who treated Ebola patients with the Red Cross in Sierra Leone was hospitalized in Australia after developing a low-grade fever, health officials said. She is being tested for the deadly virus.
The 57-year-old volunteer recently returned to Cairns, in the northeastern state of Queensland, where she has been isolating herself and checking her temperature twice daily, Jeannette Young, the state’s chief health officer, said in an e-mailed statement. Today, she reported a temperature of 37.6 degrees Celsius (99.7 degrees Fahrenheit). Results of tests for Ebola and other possible infections are expected early tomorrow.The nurse hospitalized in Cairns was identified as Sue-Ellen Kovack by the Australian newspaper. Kovack returned home two days ago, the newspaper reported.
A Turkish worker employed in Nigeria was rushed to an Istanbul hospital Oct. 8 on suspicion of Ebola, according to Hurriyet Daily,after showing signs of a high fever and diarrhea.
The 46-year-old man, whose identity has not been disclosed, returned to Turkey 10 days ago from Africa to see his family in the western province of Sakarya during the Feast of the Sacrifice holiday.The incident is the second case of a suspected Ebola patient in Turkey, after a Nigerian woman who transited through Istanbul’s Atatürk Airport while traveling from Lagos to Barcelona was rushed to hospital in mid-August.
Health officials from the German state of Saxony confirmed on Thursday that an Ebola patient had arrived in the country,according to DW,
The man, who originates from Sudan, contracted the virus in Liberia, they said, adding that he had been transported from the airport to the St. Georg Clinic in the city of Leipzig, which is located roughly 200 kilometers (125 miles) southeast of Berlin.St. Georg's Clinic is one of seven health facilities in Germany with the capability to treating highly infectious patients in isolation.Two other Ebola patients have also been flown to the Central European country in recent weeks. A World Health Organization (WHO) employee had fallen ill with the hemorrhagic fever in Sierre Leone was brought to Hamburg, where doctors were able to stabilize him and eventually release him last week.
And finally, with regard the infected Spanish nurse in Madrid (as The Guardian explains), had told health authorities at least three times that she had a fever before she was placed in quarantine.
Her first contact with health authorities was on 30 September when she complained of a slight fever and fatigue. Romero Ramos called a specialised service dedicated to occupational risk at the Carlos III hospital where she worked and had treated an Ebola patient, said Antonio Alemany from the regional government of Madrid. But as the nurse’s fever had not reached 38.6C, she was advised to visit her local clinic where she was reportedly prescribed paracetamol.Days later, according to El País newspaper, Romero Ramos called the hospital again to complain about her fever. No action was taken.On Monday, she called the Carlos III hospital again, this time saying she felt terrible. Rather than transport her to the hospital that had treated the two missionaries who had been repatriated with Ebola, Romero Ramos was instructed to call emergency services and head to the hospital closest to her home. She was transported to the Alcorcón hospital by paramedics who were not wearing protective gear, El País reported.On arrival at the hospital, Romero Ramos warned staff that she feared she had contracted Ebola. Despite the warning, she remained in a bed in the emergency room while she waited for her test results. She was separated from other patients only by curtains, hospital staff said on Tuesday.
* * *
As of yesterday...

* * *
But apart from that... "contained"
Links from Naked Capital.....
Ebola
Ebola virus: Spanish protests as nurse’s dog is put down BBC. There’s a detail in this story of general public health importance: the authorities believe the nurse became infected when removing her protective gear. That risk presumably applies to any personnel treating Ebola patients unless their facilities have an area where exterior of the protective clothing is decontaminated before they take it off. Pray tell how many US hospitals have that?
Why Ebola is a threat Ian Welsh
Brandon Smith ....
http://www.alt-market.com/articles/2354-an-ebola-outbreak-would-be-advantageous-for-globalists
An Ebola Outbreak Would Be Advantageous For Globalists
It's sad to say with such finality, but a universal fact of existence is that most of the people you meet in this life are fundamentally and functionally ignorant. Not necessarily stupid, but certainly ignorant. Ignorance comes not from a lack of intelligence, but from a denial of knowledge and truth. That is to say, ignorance takes hold when people decide to act as though they know and understand a thing, even if they do not. Ignorance prevails when a society or nation chooses to value the appearance of expertise, to value the theater of overconfidence, and to cheer for the bluster of morons rather than admit that they have unanswered questions on subjects they do not yet grasp. For nothing is worse for the self absorbed than to acknowledge that they do not know.
Entire nations have fallen throughout history because of this terrible weakness...
By extension, such ignorance is not just an inherent disease but also an easily exploitable disease. When we refuse to think critically and examine our surroundings thoroughly, we become like grazing gazelles oblivious to the predators encircling us in the tall grass. And, just as there are predatory individuals that hide amongst us, there are are also predatory oligarchs that camouflage themselves as benevolent politicos and financial professionals standing above us. Normal predators we fear, establishment predators we invite into our homes as protectors, saviors, and partners.
The disease of ignorance leaves us vulnerable to many other plagues, including literal plagues like the Ebola virus. When we take the establishment at its word concerning the threat of Ebola outbreak, we make ourselves vulnerable. When people assume that the worst could never happen to them, history shows us that it inevitably does.
The recent discovery of an Ebola infected patient in Dallas, Texas has led to reasonable concern from the general population, but mainstream media efforts along with CDC and White House spin have subdued any practical response by the citizenry. The constant droning voice of the establishment claims there is nothing to be worried about; that even if there was an outbreak in the U.S., it would be quickly squashed by highly prepared medical response teams.
First and foremost, the existence of just one Ebola infected person within America's borders indicates a likelihood of others, or the possibility of others in the near future unless policies and procedures are changed. As far as I can tell, the government has no intention of introducing rational fail-safes such as requiring mandatory quarantine for those seeking to reenter the U.S. from known outbreak regions, shutting down unrestricted travel into the country from countries with Ebola, training hospitals properly in the identification of the disease, or committing mass resources to quelling Ebola in hot zones before it reaches our shores, at least not in time to make a difference.
Secondly, the establishment also has no intention of giving the general public accurate information as to the behavior and dangers of Ebola. Those I have spoken with in the medical field including some who work within major city hospitals have related to me that the CDC has not been honest in its assessment of the probability of outbreak. For example, the CDC is consistently reminding the public that Ebola is not an “airborn” disease, and this is technically true as far as the science indicates. However, they forget to mention that it is indeed a “droplet born” disease, meaning, it can travel through the air carried in an infected cough or sneeze. The tight quarters of an airplane make for a perfect petri dish, with droplets and particulates passing back and forth through the same space and oxygen for hours at a time. The spread of Ebola is nowhere near as containable as the CDC claims.
I have been told that most hospitals are completely unprepared to fend off an outbreak of a virus as destructive as Ebola. Little to no standardized training has taken place, and some facilities are only now putting together a list of emergency procedures. Human error within the chain of care also occurs often, as we saw in Dallas, Texas, and these errors can lead to greater infection in a hospital environment.
CDC and WHO efforts in countries like Liberia have been so ineffective and halfhearted it leads one to question why their budgets are in the billions of dollars? Where is all their capital and their resources going if not to bring an unprecedented hammer down on a clearly dangerous outbreak of Ebola? Why is the virus being allowed to flourish rather than being destroyed right where it started? Where has the full force of the CDC been for the past several months while death gestates in Africa?
The one legitimate function of government, any government, is to protect the right of the people to pursue their own life, liberty, and happiness. I think stopping the invasion of mortal viruses would fall into this category. The one job our government is MANDATED to do, and it refuses to do it. Why?
I have made the point many times in the past and I'll make it here again; when a catastrophe takes place, or a crisis is imminent, ask yourself, who ultimately benefits? I believe that the lack of strong prevention response from our government, an inadequacy which is obvious to all of the health care workers I have talked with and to anyone who has the sense to do their own research, could be absolutely deliberate. I believe the spread of Ebola may be desired by certain power brokers, and here is why:
The Perfect Cover Event
I have been warning for quite some time that the banking establishment in particular is well aware that an economic collapse of incredible proportions is coming. In fact, they have done everything in their power to make one possible. This collapse, according to my research, is designed to clear the way through monetary carpet bombing for a new international Bretton Woods-style agreement which will plant the foundation of a truly global economic system centralized and controlled by a highly select few elites. Needless to say, the internationalists would prefer not to take the blame for such a calamity.
Regional or widespread war, terrorism, cyber attacks, etc, are all useful vehicles to conjure mass confusion, and can also be used as scapegoats for the eventual downfall of our economy. That said, a viral pandemic truly surpasses them all in effectiveness. All other tragedies could easily be tied to the first “domino” or “linchpin” (as Rand Corporation calls it) of Ebola transmission, but the strategy goes deeper than this...
An Act Of Nature
Even though most people are well aware of the fact that governments have been engineering biological weapons for decades, few people think political leadership would ever use them at all, let alone use them on the people they are tasked to protect. Even with the complacency and inaction of our government in terms of the response to Ebola, the general assumption by most of the American population will be that any viral outbreak is a product of nature, not of men.
Acts of nature are not things that the common man can easily rebel against. People rebel against governments and corrupt despots all the time, but not the plague. If a viral pandemic strikes, nearly everything a government does after the fact, no matter how corrupt or destructive, can be rationalized as necessary for the greater good of the greater number. If anyone does rebel, they will be labeled as pure evil, for they are now disrupting the government's ability to stop the pandemic from spreading, and thus, are partly responsible for the mass deaths that follow.
During a viral outbreak, government becomes mother, father, nurse and protector. No matter how abusive they are, most people will still look to them for safety and guidance, primarily because they have no knowledge of disease. What they do not understand, they will fear, and fear always drives the ignorant into the arms of tyrants. One should also take into consideration the fact that most globalists lean towards the ideology of eugenics and promote the concept of population reduction. A pandemic would fulfill this desire nicely...
Rationalized Economic Collapse
Who would question the event of an economic collapse in the wake of an Ebola soaked nightmare? Who would want to buy or sell? Who would want to come in contact with strangers to generate a transaction? Who would even leave their house? Ebola treatment in first world nations has advantages of finance and a cleaner overall health environment, but what if economic downturn happens simultaneously? America could experience third world status very quickly, and with it, all the unsanitary conditions that result in an exponential Ebola death rate.
The treasury, labor department, and private Federal Reserve have gone to vast lengths to skew statistics and rig markets with trillions in fiat dollars. Despite historic numbers of Americans falling off unemployment rolls, imploding shipping and manufacturing statistics, and the U.S. teetering on the edge of global “de-dollarization”, a large portion of the citizenry has been led to believe that economic recovery is assured. What they do not understand is that fiscal implosion is unavoidable, and the whole bull market is a circus designed to distract.
Amidst even a moderate or controlled viral scenario, stocks and bonds will undoubtedly crash, a crash that was going to happen anyway. The international banks who created the mess get off blameless, while Ebola, an act of nature, becomes the ultimate scapegoat for every disaster that follows.
Rationalized Travel Restrictions
If you want to lock down the movement of a population to prevent the spread of dissenting groups or ideas, I can't think of a better way than to claim it is to prevent the spread of a deadly virus. Our government and world health officials are approaching Ebola with an attitude of nonchalance right now, because prevention is NOT part of the plan. When Ebola strikes hard within our country, that is when they will finally decide that strict measures are needed. Suddenly, those borders that they could never secure before will become impassable for you and I. And traveling between states or perhaps even counties may be extraordinarily difficult. “Papers please...” will become the new mantra of petty authority.
Forced Health Measures
Do not be surprised if an Ebola vaccine of some kind suddenly appears on the market just as the situation begins to turn tragic. And, do not be surprised if said vaccine is a total sham that ends up making more people sick. Expect that forced vaccinations will take place, especially as a prerequisite for receiving treatment from CDC or FEMA hazmat facilities. Expect that these facilities will become nothing more than obscure prisons for the sick where people quietly die. Expect that every American will be required to be tested and screened, with biometric data carefully stored, beginning with airport travel (once the virus is already entrenched). The options are endless for abuse in terms of totalitarian health laws when the public thinks they could end up bleeding from every orifice and dying of liver failure.
Rationalized Martial Law
Imagine if some Americans decide they don't like being poked, prodded, tagged and bagged by the establishment. Imagine they decide to fight back, Ebola be damned. An already uphill battle becomes an epic struggle when a large percentage of the population thinks you are a monster that wants to hasten the spread of Ebola. Not that the ignorant count for much in the grand scheme of history, but waking at least some of them up in the future to the bigger threat (the globalists) is hard to do when all they can see is devilish microbes. Those who plan to combat the rise of the internationalists, as I plan to, should accept now the likelihood that the only people we will have on our side tomorrow are the people we have been able to wake up today. Martial law will be welcomed by the rest.
International Response
An international response is almost guaranteed during a major pandemic. Sovereignty will be tossed in the dirt. UN and WHO teams and perhaps even troops could accompany an aid package to the U.S. Think of the glorious propaganda, as globalists tell stories of how they “saved humanity” by surpassing the barbaric practices of national and individual sovereignty, defeated the Ebola virus (after millions of deaths, of course), and out of the ashes, the “phoenix” of global governance was born. If they succeed, imagine what the history books will say for the next several centuries.
What Do We Do?
There are no silver bullet solutions. There never have been and there never will be. People looking for them will be sorely disappointed and ill prepared after wasting so much time searching for an easy out. The only answer is for communities of people to take their own survival into their own hands and become as self sufficient as possible. This means that neighborhoods, towns, and counties will have to take precautions now to steel themselves for a pandemic event, instead of simply sitting on their hands and expecting government officials to save them.
The treatments for Ebola in most cases involve nothing more than the steady replacement of vital fluids, electrolytes and plasma until the patient's body can build up an immunity to the virus. Those with stronger immune systems before contraction are more likely to survive and beat back the disease. Government care, for the most part, is NOT going to save many people either way. That is to say, your survival will depend on you and your immune system, not them. Communities that make efforts to prevent contact and that strengthen individual immunity will have a better chance of survival than going into any government run hazmat facility. Government is not needed, and will often end up being more of a threat than the virus itself. Groups I work closely with and talk with, many with their own doctors and nurses, are already setting prevention guidelines in motion.
If you can prove you don't need the system to save you, their rationale for attempting to control you is weakened. The ignorant will still try to demonize us for our efforts, but self sufficiency is all we have in the face of this kind of storm. If we can lead by example with our own successful health standards while saving people where the establishment could not, perhaps we can turn the tide.
Zero Hedge.....
Finally, Here Come The Banks: "Ebola Is A Tail-Risk That Can No Longer Be Ignored"
Barclays' FX Research team explains why Ebola can no longer be ignored...

1. Is Ebola a significant market risk?
Before the current Ebola outbreak began in December, the disease was already notorious and fear inspiring despite having afflicted only 2,345 people in the 37 years since its discovery, nearly all of whom were in remote villages in Central Africa and 1,546 of whom died. Yet, as long as sporadic outbreaks remained contained and confined, it had little impact on the global economy or markets. The current outbreak in West Africa may be changing that.
The West African Ebola outbreak that began in Guinea is notably different from prior outbreaks in ways that significantly increase its chances of having a broader impact. In particular, Ebola’s likelihood of spreading to larger, more integrated economies has increased. It remains a tail risk, but has jumped in probability to one that can no longer be ignored.
There are several important differences between this Ebola outbreak and previous episodes.
First is its size: confirmed cases and mortalities – 4,087 and 2,071, respectively – already are greater than all prior outbreaks combined and growing at an uncontrolled pace. Including probable and suspected cases increases those numbers to 7,470 and 3,431, respectively (Figure 1), and both the US Centers for Disease Control (CDC) and the World Health Organization (WHO) believe these numbers are underestimated, perhaps by a factor of 2.5.

Second, the current outbreak is more urban than prior outbreaks, with Freetown, Sierra Leone and Monrovia, Liberia being among the hardest hit areas.
Third, and perhaps most importantly, the current outbreak is on the edge of a vast, densely populated area of 334 million people that is an ideal breeding ground for disease (Figure 3). As Robert Kaplan described it 20 years ago when its population was about half as large, “the Lome-Abidjan coastal corridor – indeed, the entire stretch of coast from Abidjan eastward to Lagos – is one burgeoning megalopolis that by any rational economic and geographical standard should constitute a single sovereignty, rather than the five (the Ivory Coast, Ghana, Togo, Benin, and Nigeria) into which it is currently divided.” Somewhat presciently, Kaplan noted this densely populated, impoverished, crime-ridden area was a perfect Petri dish for pestilence.

Figure 2 presents statistics on some of the socio-economic and health factors that make the region particularly susceptible to disease. The region’s young population – median age is 18.3 years – suffers the worst of poverty’s fellow travellers, including low literacy rates, poor access to clean water and to improved sanitation, and few health professionals and facilities. Illiteracy and residual warlordism from recent civil wars were key contributors to the rapid spread of Ebola in Sierra Leone and Liberia as health workers had difficulty educating a distrustful population on prevention, and in cases have been attacked on rumors they brought the disease. Making matters worse, Ebola has disproportionately stricken healthcare workers, reducing already low ratios to the general population.

A fourth difference is an active debate over how contagious the virus is now and what its potential to become more contagious is. Researchers have established that Ebola’s genetic structure is subject to a rapid pace of mutation and have documented numerous genetic changes to the virus, Zaire ebolavirus, one of five documented strains of Ebola, both from previous outbreaks and since the current outbreak began. The implications of these changes for the virus’s behaviour and morbidity are not yet known and will require significant further study. Health officials and researchers are not in agreement about the virus’s current and potential means of transmission. The WHO and CDC maintain that Ebola can only be transmitted via direct contact of an infected, symptomatic person’s bodily fluids with open lesions or with mucus membranes. Yet, the Public Health Agency of Canada and the Federation of American Scientists warn that aerosolized transmission, though unconfirmed in human-to-human transmission, has been documented in non-human primates and pigs.
Adding to the debate over the contagiousness of the strain of Ebola behind the current West African outbreak is its rapid expansion and higher-than-usual rate of infection of health professionals. The current outbreak is between 6.8 and 12.4 times larger – confirmed versus suspected cases – than the next largest outbreak, the first one in (then) Zaire and Sudan in 1976. As noted above, this may reflect a slow initial response combined with cultural differences between West Africa and Central Africa. But the higher rate of infection among health professionals is more difficult to explain. Through late August, the latest date for which complete statistics were available, 120 healthcare professionals had died from Ebola, or roughly 8% of confirmed, probable and suspected cases. By comparison, in the 1976 outbreak, when Ebola was an unknown new pathogen, 11 healthcare workers died from the disease, 2% of total deaths. Among the health professionals killed by the disease were five of 58 authors of the genomic study of the current outbreak, cited above, including Sheik Humarr Khan, an expert on hemorrhagic fevers and director of the Lassa fever program for the Sierra Leone Ministry of Health and Sanitation.
A more robust domestic and international response may still turn the tide of Ebola. The spread of the West African outbreak to both Senegal and to Nigeria was quickly contained and no new cases have manifest. In the last month, global attention has increased and with it resources devoted to combating the disease’s spread. Indeed, there already are signs that its pace of expansion has slowed.

Figure 4 plots the rate of growth of new Ebola infections – confirmed; confirmed and probable; and confirmed, probable and speculated – at a monthly rate between WHO situation reports (the longer time series in Figure 1 is for combined confirmed, probable and suspected cases). All three measures have fallen sharply to just under 50% per month since the surge of the late summer, when the average rate of change at a monthly rate rose to over 100%. However, this only takes the rate of expansion back to its July level, and the late summer surge may have reflected improved accounting. Furthermore, the geographic distribution of new cases continues to expand within Guinea, Liberia and Sierra Leone, and is expanding towards Côte d’Ivoire.
A strong external response may reinforce the trend of slowing expansion and ultimately contain and extinguish the West African outbreak. If it does not and Ebola’s eastward expansion continues at even the reduced current pace into the more populous countries of West Africa, the mathematics of geometric progression implies terrifyingly large numbers of cases in the not-distant future. The path of cumulative Ebola cases is projected, in log scale, in Figure 5 under two growth rate assumptions: the average rate of growth of confirmed cases since end June (66% per month) and since end August (54%). Both paths are more conservative than the CDC’s projection of 550,000 cases by January – even more so relative to the CDC’s “worst-case scenario” of 1.4 million – because the CDC includes probable and suspected cases in their starting point. But even more conservative projections that start with only confirmed cases and use the slower September growth rate suggest that there could be 1 million cases by the first week of August, 2015. If growth averaged its June-September pace, there could be 1 million cases by the second week of June 2015.

Case numbers that large raise the probability that Ebola could become endemic – that is permanently resident – in the West African population of 334 million. Beyond the human tragedy that implies for West Africa, the prospect of endemicity increases the probability of Ebola having a greater impact on the global economy and financial markets. Afflicted countries’ relatively small weight in global GDP, trade and financial markets so far has limited Ebola’s effects on global markets despite an already larger-than-SARS death toll.10 But a sustained outbreak in a larger or more globally integrated economy likely would have a significant impact on global markets.
That endemicity of Ebola to West Africa, or even a larger outbreak, greatly increases the chances of the disease breaking out to other more economically integrated economies is evident in the fact that cases have already been confirmed in Dallas, Texas and Madrid, Spain despite an outbreak of only 7,000 people in three small countries without direct air traffic to either the United States or Spain. If the projections in Figure 5 are fulfilled – much less the worse estimates of the CDC – the likelihood of Ebola spreading to other economies would rise sharply. The economic and market effects of sustained global outbreaks is another source of uncertainty, undertaken in the next question.
2. What lessons does SARS hold for Ebola?
The 2003 SARS outbreak, primarily in East Asia, is a good starting point for analysis of the potential effects on economies and on global financial markets of an expansion of Ebola outside of West Africa. But one of the lessons from the SARS experience is that it may not be an appropriate analogue for a possible Ebola breakout from Africa.
Barclays re-examined some of the lessons of the SARS episode for Asian economies in Revisiting Asia’s SARS experience, 20 August 2014. Among the lessons: 1) supply disruptions were minimal because the disease did not afflict enough people to curtail labor supply meaningfully; 2) the primary impact was a panic-driven decline in demand, especially for local services and for tourism, but there was some short-lived effect on trade and investment as decisions were delayed due to uncertainty; 3) once the disease was controlled and panic subsided, activity rebounded rapidly.
There are important differences between the SARS and West African Ebola outbreaks, however, both in current fact and in potential. SARS, an airborne respiratory virus, is more contagious than Ebola, but only about 1/8th as lethal. The greater lethality of Ebola, if its spread continues, may imply a supply effect for currently affected economies that was not present with SARS, especially in the dominant, labor-intensive agrarian sector. SARS afflicted several economies that were deeply integrated in the global economy, including Canada, China, Hong Kong, Singapore, Taiwan, and Vietnam; whereas Ebola is confined to much smaller, much less globally integrated economies. The SARS afflicted economies also benefitted from much better health statistics than do West African economies (see Figure 3). As noted in Question 1, this may explain Ebola’s rapid spread in the current outbreak.
The more interesting differences may be around potential. If Ebola continues to expand as explored in Question 1 and becomes endemic to West Africa, its then likely eruptions into the broader world also may be different from the SARS experience. First, while Ebola is not now as contagious as SARS, its greater mortality likely will inspire as much panic as SARS. But the difference with SARS would be that the persistence of a large human host reservoir would mean any panic may not fade as rapidly, particularly if it spawned sporadic mini outbreaks.
Second, the persistence of a large human host reservoir in West Africa would increase the probability that Ebola became epidemic or even endemic elsewhere in two ways: the continuous flare-ups of outbreaks would give the virus more chances to take hold elsewhere; and, as discussed in Question 1, a human host reservoir would give it greater opportunity to evolve into a more communicative, higher morbidity disease. SARS never became epidemic or endemic anywhere, and as such was not able to significantly affect the supply chain of the global economy. A sustained outbreak of a high mortality disease like Ebola in any large or important economy in the global supply chain would imply significantly larger impact than SARS caused.
3. What do you need to monitor and what could be Ebola’s effects?
As noted above, for Ebola to become a serious market risk, it needs to more acutely threaten demand or supply in larger or more economically integrated economies. Ebola’s threat to the global economy and markets would increase markedly if it either became endemic to West Africa or became more contagious and increased its rate of morbidity. But the response of larger, more economically integrated countries to any breakouts of the West African Ebola virus is likewise important.
What should investors monitor to assess the risks to markets from Ebola? In our view, three things:
1. A sustained pace of expansion within West Africa, or conversely containment and recession that eliminates the likelihood of endemicity;2. Evidence of increased contagiousness among new cases, either due to new transmission vectors (like aerosol) or a longer period of asymptomatic contagion;3. The success of countries outside of West Africa in containing the periodic cases that likely will escape the region, or already have in the case of Dallas, Texas.
Ebola’s expansion can be monitored in WHO situation reports on the West African Ebola outbreak: does the rate of infection continue to slow and remain restricted to Guinea, Liberia and Sierra Leone, or does it expand to new countries and sustain a rapid pace of expansion? Monitoring contagiousness is more difficult as it will be months before even preliminary analyses of the already documented changes in the Ebola genome are mapped to phenotypical outcomes (physical or chemical changes that determine the virus’s survival and means of replication). The sole case of Ebola in Dallas, Texas is simultaneously concerning and reassuring. There are already several well documented missteps in containment of the victims’ contacts, and yet the lack of further infections – so far – is reassuring that Ebola may be less dangerous in wealthier, healthier societies.
If Ebola becomes endemic and more contagious, its threat to the global economy and markets likely will be greater than SARS’ impact in 2003. Without endemicity in West Africa, mishandled outbreaks outside of Africa may have more temporary, SARS-like effects on local economies and markets. The greatest potential impact of Ebola is a combination of the two: endemicity and/or greater contagiousness combined with a mishandling of an outbreak outside of West Africa. That combination, for the reasons noted in Question 2, likely would have a significantly greater impact on the global economy, perhaps through both demand and supply channels, and as such on global financial markets.
Endemicity of Ebola in West Africa that spawned continuous periodic outbreaks elsewhere, or more destructively a sustained outbreak in a large or globally integrated economy, likely would lead to lower average growth with greater volatility, lowering risk free yields and increasing risk asset spreads. Those countries that best demonstrate their ability to avoid contagion, or best manage Ebola outbreaks when they occur, likely will see lower risk premia attached to their assets and higher equilibrium exchange rate values.
It must be emphasized again that endemicity of Ebola anywhere – including West Africa – remains a tail risk. But it is a tail risk that has left the fringes.
US Ebola-Fighting Troops Mission Could Last A Year; Spain Quarantines 6, Euthanizes Dog; US Patients Conditions Worsen
Africa's US commander has admitted troops will be fighting Ebola for about a year (and in direct contact with infected individuals). Both US Ebola patients conditions are worsening, as Reuters reports, Thomas Duncan is fighting for his life on a ventilator (and undergoing dialysis) and NBC cameraman Ashoka Mukpo is receiving blood from Ebola-survivor Dr. Kent Brantly. The outbreak in Spain has spread with 6 "high risk" patients under quarantine (and Excalibur the dog is set to be euthanized - raising questions about transmission mechanisms). The economic impact on West Africa continues to surge with The World Bank estimating a $32billion hit by the end of 2015.
US troops will be fighting Ebola for a year...
Thousands of U.S. troops may be living in tent cities in Liberia and supporting the fight against Ebola for "about a year" or until the deadly outbreak appears to be under control, the top military commander in Africa said Tuesday."This is not a small effort and it's not a short period of time," Army Gen. David Rodriguez, the chief of U.S. Africa Command, told reporters at the Pentagon.
Duncan is suffering...
The Ebola patient fighting for his life in a Dallas hospital is on a ventilator and a kidney dialysis machine to help stabilize his health, the hospital said on Tuesday.Liberian national Thomas Eric Duncan, the first person diagnosed with the deadly virus on U.S. soil, has also been given the experimental medication brincidofovir.
And Mukpo is receiving blood transfusions..
The first American flown back to the U.S. after contracting Ebola has donated blood to an NBC News freelance cameraman who was also diagnosed with the virus.Photojournalist Ashoka Mukpo’s family told NBC News early Wednesday that Dr. Kent Brantly was contacted by the Nebraska Medical Center and asked to give plasma.Experts hope the survivor’s antibodies will kick-start Mukpo's immune system.
As Spain quarantines another potential Ebola patient...
One more Spanish health care worker was admitted to hospital for monitoring for Ebola today, bringing to six the number of hospitalisations in Madrid where a nurse has been infected with the disease, a hospital official said.In the latest case, a nurse was quarantined at Madrid's La Paz-Carlos III hospital today morning as a precaution, a spokesman for the hospital said.Another nurse had been admitted to the hospital with a fever yesterday night and put in quarantine for monitoring, he added, confirming Spanish media reports.Three other people had been placed in quarantine at the hospital for monitoring after a nurse who works there was diagnosed with Ebola on Monday in the first case of transmission of the disease outside of Africa.The woman, identified by Spanish media as Teresa Romero, a woman in her forties, had cared for two elderly Spanish missionaries who died from the virus following their return from west Africa.Among the six people hospitalised was the woman's husband, considered at "high risk".
Not even man's best friend is safe (as CBC reports),
Ebola's victims may include a dog named Excalibur. Officials in Madrid got a court order to euthanize the pet of a Spanish nursing assistant with Ebola because of the chance the animal might spread the disease.At least one major study suggests that dogs can be infected with the deadly virus without having symptoms. But whether or how likely they are to spread it to people is less clear.Lab experiments on other animals suggest their urine, saliva or stool might contain the virus. That means that in theory, people might catch it through an infected dog licking or biting them, or from grooming."Clearly we want to look at all possibilities. We have not identified this as a means of transmission," said Dr. Thomas Frieden, director of the U.S. Centers for Disease Control and Prevention.
* * *
And The World Bank is concerned at the economic costs...
The deadly Ebola epidemic could deal a USD 32 billion-plus blow to the West African economy over the next year if officials cannot get it under control, the World Bank warned today.If efforts to halt its spread out of a three-country core -- Liberia, Sierra Leone and Guinea -- are not successful by December, the entire region faces a real threat of economic catastrophe, the Bank said in a new report."In broader regional terms, the economic impacts could be limited if immediate national and international responses succeed in containing the epidemic and mitigating aversion behavior," it said."If, on the other hand, the epidemic spreads into neighboring countries, some of which have much larger economies, the cumulative two-year impact could reach US$32.6 billion by the end of 2015."
* * *
It appears Ebola is not contained...

Evening tweets.... 2nd case in Texas ?

Report: Man who may or may not have had contact with Dallas Ebola patient now exhibiting similar symptons http://hotair.com/?p=1519501
Is this a confirmed 2nd case of Ebola in the US? We'll ask the Secretary of Homeland Security: http://cnn.it/1v0JxLU
U.S. will screen for Ebola at:
New York’s JFK
Washington Dulles
Newark Liberty
Chicago O’Hare
Atlanta Hartsfield
http://bloom.bg/1rXKn9R
 CBS This Morning
CBS This Morning 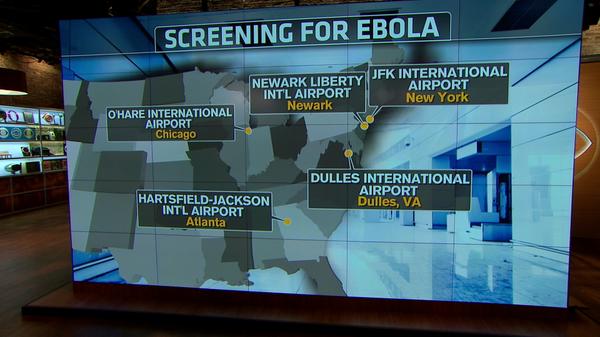
 Lee Pacchia
Lee Pacchia
whelp. RT @MotherJones: Research shows Ebola can be found in survivors' semen for weeks/months after recovery http://bit.ly/ZetNbE

Top news story
 PB PLUS OIL AND GAS
PB PLUS OIL AND GAS
http://ow.ly/CqfD3 Prime Minister urges Spain to stay calm http://ow.ly/CqfD4 BB PIN: 2ab2cc5b

Families of healthcare workers may lose their breadwinner. MT @AlaskaiMJohnson Hospital workers protest #EbolaLiberia

Morning Tweets ....
 All News World
All News World
[AP] Sierra Leone strike halts burial of Ebola dead http://apne.ws/1vUb0wN
Spanish Ebola nurse reported symptoms many times before being quarantined http://www.theguardian.com/world/2014/oct/08/spanish-ebola-nurse-symptoms-quarantine …

AFRICA EBOLA MISSION US military personnel to handle blood samples: Experimental drug the 'best choice' for A... http://tinyurl.com/p388tyg

 Marilyn Thompson
Marilyn Thompson
Some Ebola experts worry virus may spread more easily than assumed http://fw.to/gOV2dxK

Top news story
 Telegraph World News
Telegraph World News
Spain Ebola case: Screen and sticky tape to protect against virus http://tgr.ph/1qg64hm
Britain must start screening for Ebola, says Home Office minister
http://ind.pn/1BRp4cz


Ebola cost to W.Africa economy could top $32 bn: World Bank http://f24.my/1qgQVMN

No comments:
Post a Comment